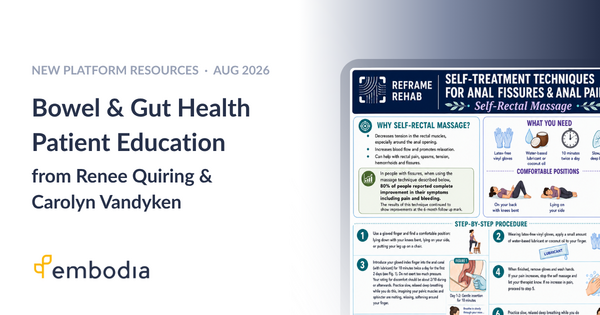
Bowel & Gut Health Patient Education for Your Clinic
New on Embodia: a Reframe Rehab collection of bowel and gut health patient education from Carolyn Vandyken and Renee Quiring, plus clinical assessment resources for Year of Mentorship participants.

Where Physical Therapy Meets Yoga Therapy and Pain Science
An upcoming live series 'From Bodily Knowledge to Intuitive Movement' with Sherry Brourman bridges physical therapy, yoga therapy, and pain science.
Directional Preference: What's Happening in the Tissue?
What's really happening at the tissue level with directional preference and centralization? A look at MDT theory, evidence, and what's still unknown.
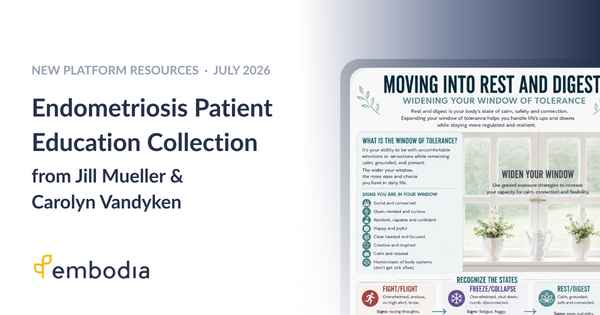
Endometriosis Patient Education Resources for Your Clinic
Twelve plain-language endometriosis patient education resources by Jill Mueller of EndoTogether are now in Embodia's library, all ready to share with your patients.

The Pain I Thought Was Normal: An Endometriosis Physiotherapist's Story
Pelvic health physiotherapist Jill Mueller shares her own endometriosis and fertility journey, and how pain science changed how she treats patients today.
What's New on Embodia: July 2026
Discover what's new on Embodia in July 2026! New calendar warnings for incomplete questionnaires and consent forms, easier location scheduling, an expanded consult page toolkit, and new climbing-specific exercises in the library.

Heavy Slow Resistance Training for Tendinopathy: Achilles, Patellar & Elbow
Heavy Slow Resistance (HSR) training is the evidence-based gold standard for chronic tendinopathy: covering Achilles, patellar, and elbow (tennis elbow) tendon pain. Learn the protocol, the research, and how to apply it in practice.
What's New on Embodia: June 2026
Discover what's new on Embodia in June 2026! Two exciting features just released - Questionnaire analytics and AI DocBuilder designed to save you time and provide greater insights into your clinical practice

Endometriosis in Clinical Practice: Two Courses Every Pelvic Health Clinician Should Know About
Endometriosis affects 10% of people born with a uterus — and many present first to physiotherapy. Discover two clinical courses by Jill Mueller on endometriosis, low back pain, and biopsychosocial treatment, available now on Embodia.

Dance Medicine: Scoliosis, Male Dancers & Artistic Athletes
Dance medicine clinician? Learn about scoliosis prevalence in dancers, male dancer injury profiles, and the clinical tools shaping this emerging field.
Pelvic Health Intake Forms, Outcome Measures & Chart Templates in Embodia
Embodia includes a full library of pelvic health intake forms, outcome measures, consent forms, and chart templates — ready to use or customize for your clinic.
Whole-Person Pelvic Health Patient Education for Your Clinic
Explore Carolyn Vandyken's whole-person pelvic health patient education on Embodia, covering bladder, prolapse, persistent pain, and pain science for your HEP.